First up thank you Giles for popping something of a nudge on bluesky about weeknotes. Here’s my weeknotes.
At work
As mentioned last time I’m now part of a team working on First Contact™.
To recap:
Every day, patients and the people who care for them seek help from the NHS for new or recurring health problems.
Often they don’t know the right place to start, how urgent their problem really is, or what to expect.
When their needs aren’t met on first contact, some people:
- keep trying the same service
- try multiple methods that don’t join up
- give up and don’t get the help they need
For patients, poor, disconnected experiences can contribute to worsening health problems and avoidable harm.
For the NHS, this creates inefficiency, wastes valuable resources, and impedes access to equitable, timely, appropriate care.
I’ve been writing our newsletters to share what we’re up to within the org, and I’ll take this opportunity to steal a taster…
We can be out of sync with patients’ sense-making behaviour
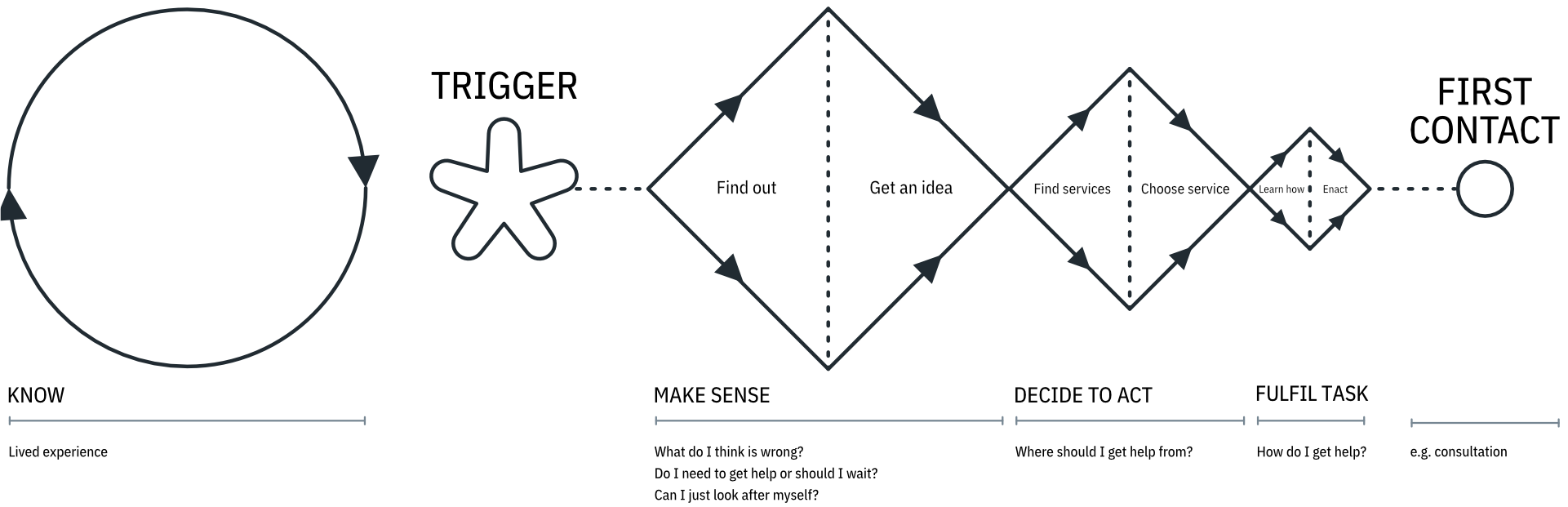
People go through a series of stages in seeking out a “first contact” with healthcare:
- Know: people’s lived experience, learned “formulas” of how and where to get help, and their current situation heavily influences how they make sense of their symptoms
- Trigger: the change in how someone feels, for whatever reason (illness, injury, etc.) that starts the process
- Make sense: people may well self-care and wait and see, talk to their friends, family and community, and do their own research (such as web searching for information)
- Decide to act: if they’re not getting better, people can ‘decide to act’ which is likely to involve the need to talk to someone. We refer to this as a ‘gear change’ – because once this point is reached, people are not satisfied with information alone
- Fulfil task: the act of trying to achieve the chosen first contact – for example making an appointment or visiting a place of care
Each one of these stages represents a tightening of focus, from the generalised and investigative to the very specific and task-oriented.
Problem: our products and services are often out of sync
For example:
- presenting information and self-help after people have decided they need to get help from an NHS service
- attempting to push people to other services after they have decided which service they need (and maybe after they physically arrived)
- confusing people with messy and sometimes circular routes to fulfil their chosen task – trying to book an appointment might be possible over multiple channels (including multiple overlapping digital ones), each route possibly having opaque eligibility criteria or a lack of clear guidance
Opportunity: what if our products and services deliberately synced with these stages of behaviour?
For example, could we:
- continue to provide and improve trusted content to help people know and make sense of their health?
- provide comprehensive and personalised service information to better help people decide where to seek help if they need it?
- ensure people can fulfil their tasks by providing clear methods to achieve those tasks, along with clear guidance about how to interact with any given service?
A fair part of me can imagine the eye rolling and groaning. As an NHS Alpha alumni I feel this pain – and the Alpha was far from the first of such familiar imaginings.
So what’s different now? I’m honestly not sure.
One thing I try to remember is that this stuff simply takes a horribly long time. Ben’s post here is one thing I read that helped me keep it all in perspective:
“Being pragmatic (you can’t achieve everything today), while still being optimistic (the bigger picture is still worth caring deeply about).”
One thing that may prove to be the big difference in time: the merger into the New NHS England means that NHS Digital as-was has graduated from comissionee to partner.
Oh is that what I do now?
I’ve been part of my new team for a few months now, and I’m often troubled with thoughts of “just wtf am I bringing to this?”
I’ve always thought of myself as someone who makes stuff of one sort or another, and over the decades that’s mostly become online things. My comfort zone seems to be “interaction of whatever flavour” more than anything else.
This new work is a lot wider ranging, and operates at so many zoom levels. The spaces we’re looking at are horribly complex and the challenge is massive. There’s no way we’re going to “make a digital thing” and magically solve it all.
All the words in front of “design” here are words like “service”, “systemic”, “organisation”, “transition“… So I’ve been struggling with just what I bring to the party, especially as I never really figured out a made-up job title for myself that felt realistic.
Luckily the fortnightly NHS design huddle had Dan Hill giving a talk about strategic design. Thanks to everyone involved in setting that up (and the huddle for that matter).
Something in Dan’s stories of what “the work” can be made me feel a lot better. Genuinely trying to approach big problems is a mixed bag of disciplines, and while we all have our specific bits of expertise, the magic is in the blend.
I guess what’s weird is this new work feels a lot like “consultancy” whilst (thankfully) being in-house. I feel like that’s a rarity in gov land?
Always good to end a post with a tangle of ill thought through waffle. I will ponder this a bit more. Until next time!